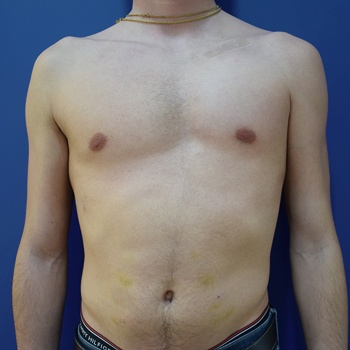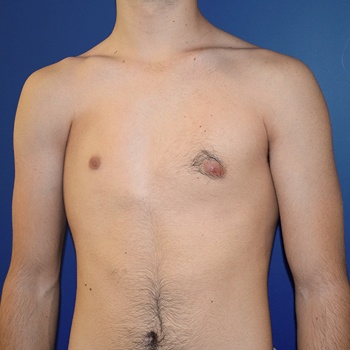
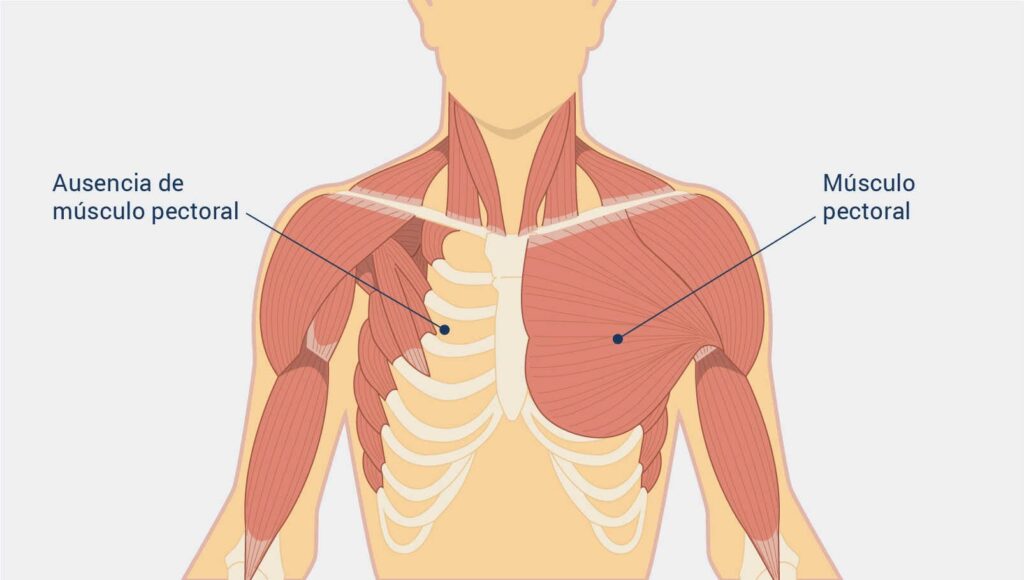
Poland syndrome, also called Poland syndactyly, Poland sequence, or Poland abnormality, is a rare birth defect characterized by the absence (hypoplasia) or underdevelopment (agenesis) of the pectoralis major muscle on one side of the body. .
Sometimes accompanied by malformations of the hand. “Webbing” (fusion) of the fingers (cutaneous syndactyly) of the hand on the same side. It is more common on the right side of the body. In 70%, is more frequent in men than in women in a proportion of 75% -25%.
In 1841, Alfred Poland, a 19-year-old medical student at Guy’s Hospital (London) published the classic description of the syndrome that bears his name. It affects one in 20,000 / 32,000 live births.
In 15% of cases Poland syndrome coexists with Moebius syndrome, which is characterized by facial paralysis, inability to smile or frown, or move the eyes from side to side.
The cause of Poland syndrome is unknown. However, a disruption of embryonic blood from the arteries below the clavicle (subclavian arteries) around the sixth week of management (46th day of embryonic development) is the prevailing theory. This theory is reinforced by presenting patients, in some cases, vascular alterations and Klippel Trenaunay syndrome.
These deficiencies are largely aesthetic, with the most common (simple) form presenting as unilateral absence of the sternocostal head of the pectoralis major muscle. The deformity can also be complex, with ipsilateral absence of ribs, axillary fold, and distortions of the hemitorax. The complex may also incorporate a variety of ipsilateral trunk defects and upper limb defects, including agenesis of the anterior portions of ribs two to five, deformity of the sternum, and absence of latissimus dorsi, serratus, external and internal abdominal obliques. The breast tissues may be small or absent, and the areola and nipple complex may be small, slightly pigmented, and displaced towards the armpit.
In the case of women, the simplest cases can be successfully treated with a breast prosthesis. However, this option can accentuate subclavicular hollowness and, due to the natural narrowness of the parasternal tissues, the implant can migrate to this space. That causes a high malposition. Adjuvant breast implant treatments may include a silicone implant that repairs the chest contour and customized with CT, a TRAM or DIEP flap, and / or a latissimus (latissimus dorsi) muscle transfer, all of which can provide shape and volume to the upper poor wall.
Fat grafting is also a good option to hide the contour of the implant and achieve better symmetry. Another option is the transfer of the latissimus dorsi muscle, a technique that is used when we need to disguise the prosthesis or the expander. Its main advantage gives an adequate shape to the axillary area. The downside is that sacrificed muscle can atrophy in the long run, losing volume.
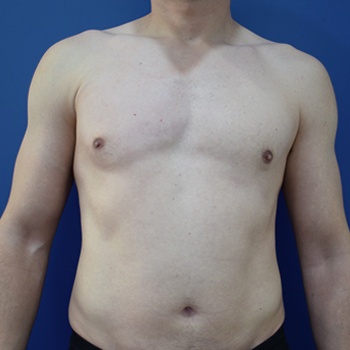
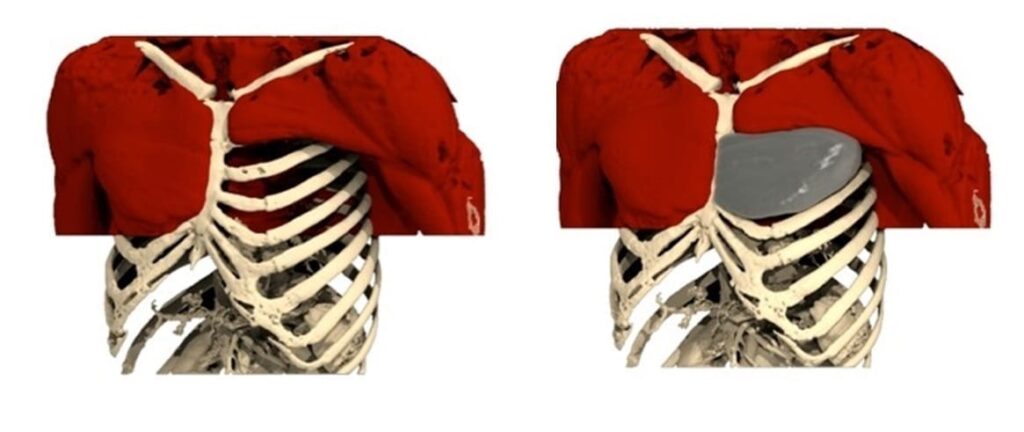
In men, the goal is to replace the missing pectoral muscle, and the best technique is to transfer the latissimus muscle to the chest. Although this is considered to be the best option, most patients do not accept using a healthy muscle for this, so in these cases we use a pectoral implant. We currently use custom implants.
We are the only Spanish reference center in Anatomik Modeling. The Anatomik Modeling reference centers have received theoretical and practical training on the computer construction of 3D implants and the different intervention techniques (pectus excavatum, Poland syndrome or other lack of muscles). These centers already carry out different types of interventions.
Fat grafting can be used to disguise the inevitable implant edges that can be seen subcutaneously and to fill in the axilla, which is not corrected by the implant. .
In patients with excess fat in the abdomen and in the healthy chest, autologous fat is obtained from these areas, so its appearance is improved by eliminating excess tissue, and using this autologous fat for further contouring.
In complex cases where there are missing ribs, the defect is treated with a synthetic mesh and the implants are not used because there is no firm bottom. In these cases, autologous tissues are the option of choice for reconstruction.
EXCELENTETrustindex verifica que la fuente original de la reseña sea Google. Maravillosa experiencia con la Doctora Salvador!!!Trustindex verifica que la fuente original de la reseña sea Google. Estic encantada! Son els millors!Trustindex verifica que la fuente original de la reseña sea Google. Muy profesionales. El trato es atento y cercano. Los resultados óptimos. He quedado muy satisfecho, los recomiendo totalmente.Trustindex verifica que la fuente original de la reseña sea Google. Es la mejor clínica. Yo fue operado por el Dr. Benito. Durante mucho tiempo elegí una clínica y un médico, dudé. Pero tuve mucha suerte, ¡caí en manos de oro! Estoy muy contenta con el resultado inmejorable. El doctor es un especialista muy atento y elegante. Todo el personal de la clínica es muy agradable. ????????✨????Trustindex verifica que la fuente original de la reseña sea Google. Muy buena clínica, la doctora Salvador explica todo de manera que sabes que estas en buenas manos.Trustindex verifica que la fuente original de la reseña sea Google. Espectacular resultado gracias al dr.benito y a su equipo????Trustindex verifica que la fuente original de la reseña sea Google. Hace más de 15 años que confío en el doctor Jesús Benito. Un gran cirujano y una persona encantadora. Gracias por todos los cuidados !!!!Trustindex verifica que la fuente original de la reseña sea Google. Muy agradecido al Dr Benito por la confianza que se gana y que te ayuda a tomar decisiones. Muy satisfecho con su profesionalidad y los resultados. Y muy contento con su equipo por lo cómodo y fácil que te hacen todo.
He worked at the Hospital Clínic in Barcelona as a specialist in Plastic and Reconstructive Surgery for 16 years.
Fifteen years ago, together with two other professionals, he founded Antiaging Group Barcelona, at the forefront of Aesthetic Medicine and Surgery. He has developed professionally in the field of care, research and teaching, being his fields of interest facial surgery, breast surgery and body contouring with implants.
In breast surgery he is a specialist in transaxillary breast augmentation and secondary breast surgery. He has introduced the use of ultrasound in Plastic Surgery and recently the use of 3D implants in thoracic malformations.

The surgery is performed under general anesthesia. After surgery, it is common for the patient to experience some pain and discomfort in the incision area, but this can usually be controlled with pain medication and other postoperative care measures.
Every patient is different and the experience of pain can vary depending on factors such as individual pain tolerance and the type of surgery performed. As a surgeon, we will work closely with the patient and the healthcare team to minimize any discomfort during and after the procedure.
It is important for patients to understand that surgery for Poland’s syndrome is an invasive procedure that requires adequate recovery time. Ensuring that the patient is comfortable and has a comprehensive postoperative care plan is an important part of the treatment process.
Like any other surgery, there are some risks associated with the procedure. Some of the most common risks include bruising, infection, excessive bleeding, noticeable scarring or even complications with the anesthesia used during surgery.
However, with a qualified and experienced surgeon, the risks are minimized and the benefits of surgery for Poland syndrome far outweigh the potential risks. It is important to discuss any concerns you have with your surgeon and follow aftercare instructions carefully to help minimize risks and ensure a quick and smooth recovery.
Medical Quality







Follow us